
Blog/News
What is hematuria?

The evaluation of microscopic hematuria is one of the most common reasons a patient is sent to see a urologist. The big three things we look for are kidney tumors, bladder tumors or stones. The most common evaluation is a non contrasted Ct scan and cystoscopy (looking into the bladder with a scope). Benign reasons for blood in the urine include irritation of the urethra in a female and the vascular lining of the prostate through which urine passes. Even the evaluation is usually negative, because blood in the urine can represent an early sign of malignancy, it is usually evaluated to assure there is no asymptomatic underlying cause.
In the picture above even though the urine appears clear there can still be significant microscopic blood in the specimen that the patient cannot see and also causing no symptoms.
Hematuria-should you be concerned?
Who was François Gigot de la Peyronie?
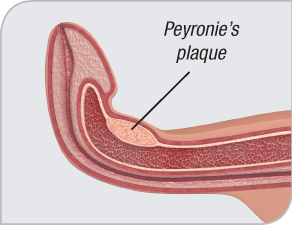
Peyronie’s disease is where plaques (segments of flat scar tissue) form under the skin of the penis. These plaques can cause the penis to bend or become indented during erections. The plaques can often be felt through the skin, and can also be painful.
Alternatives to Viagra?

From MNT
Alternatives to Viagra: Pills, Herbal Remedies, and Other Treatments
Last reviewed: Mon 28 November 2016
Viagra is a well-known drug for the treatment of erectile dysfunction, a distressing and common condition.
There are many alternatives to Viagra, which can improve or reverse the symptoms of erectile dysfunction. These options include drugs, medical treatments, lifestyle changes, and alternative remedies.
Contents of this article:
What is Viagra?
![[man looking worried]](https://i0.wp.com/cdn1.medicalnewstoday.com/content/images/articles/314/314348/man-looking-worried.jpg)
Erectile dysfunction can be distressing, but there are solutions.
Viagra was developed in the United Kingdom. In 1998, the American pharmaceutical company, Pfizer Inc., put it on the market.
The generic name for Viagra is sildenafil. The trade name is Viagra, and the drug also goes by the name of Revatio. Viagra works by slowing down the action of PDE5, an enzyme that works in the tissues of the penis.
The PDE5 enzyme breaks down a substance that is responsible for blood flow in the penis. Inhibiting PDE5 increases blood flow to the penis. This helps men to achieve and maintain an erection.
However, sildenafil can only assist in maintaining an erection if the penis is physically stimulated. Without a physical stimulus, sildenafil cannot cause an erection.
Common side effects of Viagra, or sildenafil, include headache, facial flushing, indigestion, nasal congestion, and a blue tint to the vision.
What is erectile dysfunction?
If a man is unable to get or keep an erection that is firm enough to engage in sex, does not achieve an erection at all, or loses an erection during sex, this can signal erectile dysfunction.
Erection problems are common, and they affect almost all adult men at some time. However, an ongoing issue that frequently affects erectile function may be classed as erectile dysfunction.
Figures indicate that erectile dysfunction affects over 600,000 men in the United States each year. Although the frequency of this problem increases with age, it is not confined to older adults.
Causes of erectile dysfunction
Erectile dysfunction can result from factors that are medical, psychological, emotional, or a combination of these.
Medical conditions that are linked with erectile dysfunction include:
- High blood pressure
- Diabetes
- Heart disease
- Atherosclerosis, when plaque builds up in the arteries
- Kidney disease
- Multiple sclerosis
- Peyronie’s disease, where scar tissue forms in the penis
- Injury to the penis, prostate, bladder, pelvis, or spinal cord from surgery or other means.
Psychological issues that contribute to erectile dysfunction include anxiety, depression, guilt, stress, and low self-esteem.
Lifestyle choices that have been linked to erectile dysfunction include:
- Alcohol or drug use
- Excess weight
- Lack of exercise
- Smoking.
When to see a doctor
As erectile dysfunction is a medical problem, cases that persist for several weeks or more should be seen by a doctor. This is particularly important for those who suspect their erectile dysfunction may be related to another cause, such as heart disease or diabetes.
Some prescription medications are linked to erectile dysfunction. Those taking certain prescribed drugs may wish to discuss possible side effects and alternatives to these medications with their doctor.
Drug alternatives to Viagra
There are several alternatives to Viagra available to men with erectile dysfunction.
Oral medications
Oral drugs, including Viagra, are frequently the first course of treatment offered to men with erectile dysfunction.
Alternative PDE5 inhibitors to Viagra, only available by prescription, are:
- Vardenafil: Sold under the brand names Levitra and Staxyn, this drug is available in tablet and disintegrating tablet form. To be effective, it should be taken an hour before sex. It can be effective for up to 7 hours.
- Tadalafil: Sold under the brand names Adcirca and Cialis, tadalafil can be taken 1 to 2 hours before sex. These tablets are effective for 36 hours.
- Avanafil: Marketed in the U.S. as Stendra, avanafil tablets can be taken 15 to 30 minutes before sex and last up to 6 hours.
Non-oral drugs
Alternatives to oral medications include:
- Penile self-injections: Medications such as alprostadil, papaverine, and phentolamine can be injected directly into the side or base of the penis. These can help achieve or maintain an erection for up to 40 minutes.
- Urethral suppository: Very small alprostadil suppositories can be placed in the penile urethra using a special applicator. This stimulates an erection to begin within 10 minutes, which can last for up to 60 minutes.
- Testosterone replacement: This treatment may be suggested for those whose erectile dysfunction is linked to low levels of testosterone. The testosterone hormone can be delivered by a variety of methods including injection, patch, or oral medication.
Other medical treatments
There may be some men for whom medication is unsuitable, either because of other medical conditions or another reason. In these situations, other medical treatments may be suggested.
Vacuum erection devices are hollow tubes, also known as penis pumps. They are attached to a hand- or battery-operated pump and work by drawing blood into the penis. They help to achieve an erection that can be maintained using a tension ring.
Implants are inflatable or bendable rods that are surgically implanted into the erection chambers of the penis. This type of treatment is usually only recommended after trying other options first.
All of these treatments must be delivered by a qualified healthcare professional.
Dietary supplements and herbal remedies
Several dietary supplements, herbal preparations, and food products are sold as remedies for erectile dysfunction.
![[ginseng root]](https://i0.wp.com/cdn1.medicalnewstoday.com/content/images/articles/314/314348/ginseng-root.jpg)
Ginseng may help in cases of erectile dysfunction.
Some of the better-known alternative treatments, which have shown positive results in small studies and are generally considered safe, include:
- DHEA
- Ginseng
- L-arginine
- Propionyl-L-carnitine.
However, consumers should be careful when purchasing or consuming any alternative products, including those that claim to be herbal versions of Viagra.
The U.S. Food and Drug Administration (FDA) have issued several statements warning consumers about the safety of such goods. They say these products may contain hidden synthetic chemicals or other ingredients which could be harmful. There has not been enough research to support the usage of these supplements fully.
According to the FDA, lab tests show that nearly 300 of the supplements or foods marketed to enhance sexual function contain undisclosed drug ingredients. Anyone who is using a supplement must let their doctor know.
Lifestyle changes for erectile dysfunction
Certain lifestyle choices can contribute to erectile dysfunction in some men. Research indicates the condition may be successfully reversed in some situations by focusing on lifestyle factors.
The following changes may be helpful for those with erectile dysfunction:
- Eating a balanced diet: Some research suggests that eating flavonoid-rich foods, such as blueberries, strawberries, blackberries, and citrus fruits, can reduce erectile dysfunction in both young and middle-aged men.
- Maintaining a healthy body weight: Being overweight or obese can cause or worsen erectile dysfunction.
- Engaging in regular exercise: Physical activity can benefit those with erectile dysfunction in several ways. It improves circulation, reduces stress, and it contributes to a healthy body weight.
- Quitting smoking: Research indicates a strong link between the intensity of cigarette smoking and the degree of erectile dysfunction. Stopping smoking can improve erectile dysfunction in many smokers.
- Avoiding too much alcohol and illicit drug use: Drinking too much, or taking illegal drugs, can affect sexual function in men. Smoking marijuana can cause erectile dysfunction.
- Seeking help for psychological or emotional issues: Addressing stress, anxiety, depression, and other types of emotional distress can improve or resolve symptoms.
A medical professional can give the best advice for men who are experiencing erectile dysfunction.
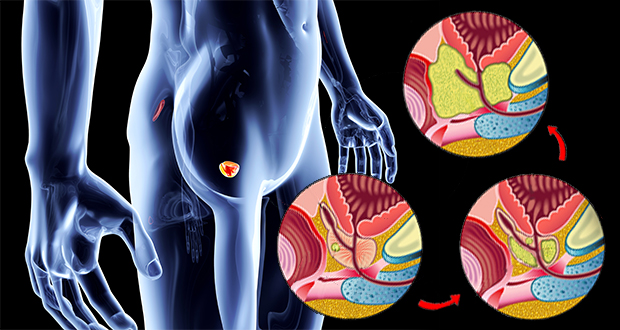
Does surgical treatment of BPH (benign enlargement not prostate cancer) cause sexual dysfunction?


Patient’s will commonly confuse the side effects of the surgery of prostate enlargement (difficulty voiding, frequency, small and slow stream, getting up at night) with that of prostate cancer surgery (leakage of urine and deterioration of sexual function).
This is not surprising as in general terms a surgical therapy is being done to the prostate and you’d think the side effects would be similar. However, in cancer surgery the entire gland is removed and in prostate enlargement the channel through the prostate where the urine flows is opened. As a result in BPH surgery (TURP, Button vaporization, GreenLight Laser) opens the channel to improve voiding but does not affect the continence mechanism or the nerves that impact potency. Surgery of the prostate for enlargement does cause retrograde ejaculation (the fluid at time of ejaculation does not come out at all or not as forcibly) but this was not found to have any impact.
The following study confirms this.
Surgical Management of BPH Does Not Reduce Sexual Function
Urology – August 1, 2006 – Vol. 21 – No. 12
Surgical management of BPH does not result in poorer sexual function, nor is there a difference between HoLEP and TURP.
Article Reviewed: Impact on Sexual Function of Holmium Laser Enucleation Versus Transurethral Resection of the Prostate: Results of a Prospective, 2-Center, Randomized Trial. Briganti A, Naspro R, et al: J Urol; 2006; 175 (May): 1817-1821.
Does a second opinion help if you have been diagnosed with prostate cancer?
I have always thought a second opinion is never a bad idea. However, maybe it just fortifies your initial intuition. Read on.
Visit ProstateCancerSecondOpinion-An excellent tool in the Decision Making Process
Do second opinions matter in prostate cancer care?
Adapted Media Release
Published: Monday 7 November 2016
A new analysis indicates that many men with prostate cancer obtain second opinions from urologists before starting treatment, but surprisingly, second opinions are not associated with changes in treatment choice or improvements in perceived quality of prostate cancer care. Published early online in CANCER, a peer-reviewed journal of the American Cancer Society, the findings also explore motivations for seeking second opinions, and suggest that second opinions may not reduce overtreatment in prostate cancer. Continue reading Does a second opinion help if you have been diagnosed with prostate cancer?
Do cranberry pills prevent bladder infections?


November is Bladder Health Month. Check out Pintrest!


What is hematuria?

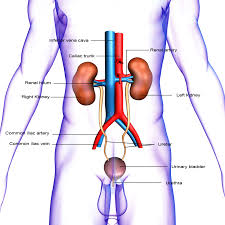
Hematuria (blood in the urine) is a very common disorder evaluated by the urologists at Northeast Georgia Urological Associates. Contact us for an appointment and we’ll get to the bottom of it.


Ben Stiller goes public about prostate cancer treatment.
Prostate cancer does not discriminate.
